A Retrospective Audit of Pancreatectomy Surgery and Diabetes (#298)
Background: Post-pancreatectomy diabetes is defined as endocrine pancreatic insufficiency occurring after surgical resection of the pancreas, leading to new onset diabetes or worsening glycaemic control in patients with pre-existing diabetes1. Poor glycaemic control may result in increased length of stay[LOS]2. We hypothesised that early, effective collaboration between Endocrinologists and Upper Gastrointestinal Surgeons would lead to reduced peri-operative diabetes-related complications and reduced LOS in these patients.
Aim: To evaluate patient outcomes and extent of physician-surgeon collaboration in managing glycaemic control in patients pre and post-pancreatectomy surgery.
Methods: We conducted a de-identified retrospective analysis of patients presenting to our hospital for pancreatic resection between 2012-2015, using data collected from the Department of Surgery electronic database and medical record charts. Data collected included: age, gender, reason for surgery, surgery type and peri-operative glycaemic management. We divided patients into three groups: patients with diabetes pre-surgery(Group1), patients who developed diabetes post-surgery(Group2) and patients who did not develop diabetes in hospital(Group3). We evaluated the involvement of the Endocrine team, development of immediate complications (DKA, hyperglycaemia), LOS and post-discharge management.
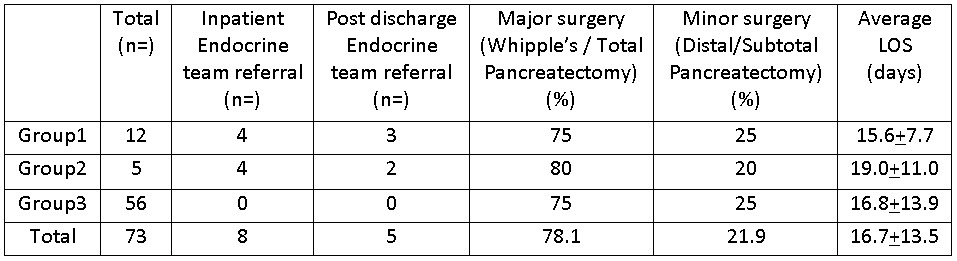
Results: There were 73 patients: mean±SD age 65.7±10.4 years with 46.6% male. Presentations were: 57 for pancreatic cancer, 6 for intra-ductal papillary mucinous neoplasms and 10 ‘other pathologies’. Surgeries were: 48 Whipple’s procedures, 9 total pancreatectomies, 10 distal pancreatectomies, and 6 subtotal pancreatectomies. For Group1(n=12), pre-operative therapy was oral hypoglycaemics[OHA](6), insulin(3) and OHA+insulin(3) and discharge therapy OHA(2), insulin(7), OHA+insulin(3). We found no evidence of pre-operative physician-surgeon collaboration. Sixteen patients(21.9%) developed hyperglycaemia post-surgery, 9 requiring insulin infusion, with no cases of DKA. Eight patients had involvement of the in-hospital diabetes team. The Table provides additional outcome data.
Conclusions: There was no evidence of pre-operative collaboration. Addition of the endocrine team to the existing multidisciplinary tumour group membership may enable collaborative development of improved referral and management pathways.
- 1. Johns Hopkins Diabetes Guide (2015) Post-Pancreatectomy Diabetes. Accessed January 18 2016, from http://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_Diabetes_Guide/547123/all/Post_Pancreatectomy_Diabetes
- 2. King, J., Kazanjian, K., Matsumoto, J., Reber, H. A., Yeh M. W., Hines, O.J., Eibl G. Distal pancreatectomy: incidence of postoperative diabetes. (2008). Journal of Gastrointestinal Surgery. 12(9):1548-53. doi: 10.1007/s11605-008-0560-5.